

Comments from Moderna CEO Stéphane Bancel on Mornings with Maria, as well as a press release from the company, demonstrate why the current shots given to protect against COVID-19 are analogous to the flu shots rather than the vaccines we receive as children that protect us against the measles and other diseases for a lifetime. The rapidly accumulating data makes the idea of vaccine mandates and passports absurd.
First, recent data from the U.K., Israel, and the CDC demonstrate that while the shots seem effective at reducing COVID-19 illness severity and duration, they do not prevent all infections, which would classify them as a therapeutic rather than an inoculation. It appears that the immune response generated by the vaccines cannot prevent the virus from replicating in all patients or for a significant period of time.
The concept of boosters has come up in several countries. Israel is currently using the original Pfizer formulation to provide boosters to at-risk patients after finding a decline in efficacy over time. Their last analysis placed the effectiveness of Pfizer’s vaccine at preventing infection at 39%, with time since full vaccination appearing to affect the level of protection. Those vaccinated in January only maintain 16% effectiveness from infection with the Delta variant. The Health Ministry’s data shows a decline in efficacy over time.
Recommended: Preliminary Data From Israel Suggests Durable Immunity to the Delta Variant in Recovered COVID-19 Patients
When Bancel spoke to Maria Bartiromo, he was clear on the need to develop boosters for specific variants. He predicted this could be available to some segments of the population—but not everyone—as early as September, which makes vaccine passports and mandates untenable. The company’s press release makes the case that COVID-19 vaccines are like the flu shot, only stronger.
According to the CDC, a flu shot is “a flu vaccine given with a needle, usually in the arm. Seasonal flu shots protect against the three or four influenza viruses that research suggests may be most common during the upcoming season.” The agency collects surveillance data on viruses to determine the formulation. If you read the agency’s description of influenza viruses, it is very casual in describing the mutations the virus undergoes because they expect it:
Currently circulating influenza A(H1N1) viruses are related to the pandemic 2009 H1N1 virus that emerged in the spring of 2009 and caused a flu pandemic (CDC 2009 H1N1 Flu website). This virus, scientifically called the “A(H1N1)pdm09 virus,” and more generally called “2009 H1N1,” has continued to circulate seasonally since then. These H1N1 viruses have undergone relatively small genetic changes and changes to their antigenic properties (i.e., the properties of the virus that affect immunity) over time.
Of all the influenza viruses that routinely circulate and cause illness in people, influenza A(H3N2) viruses tend to change more rapidly, both genetically and antigenically. Influenza A(H3N2) viruses have formed many separate, genetically different clades in recent years that continue to co-circulate.
Influenza B viruses are not divided into subtypes, but instead are further classified into two lineages: B/Yamagata and B/Victoria. Similar to influenza A viruses, influenza B viruses can then be further classified into specific clades and sub-clades. Influenza B viruses generally change more slowly in terms of their genetic and antigenic properties than influenza A viruses, especially influenza A(H3N2) viruses
So, the CDC predicts which type of each virus may circulate every year and develops a shot to address specific variants. Our healthcare experts did not eradicate it and never expected to. It is now endemic. SARS-CoV-2 will be no different long term, and Moderna’s release essentially acknowledges this:
Our mRNA platform allows for rapid design of vaccine candidates that incorporate key virus mutations, potentially allowing for faster development of future alternative variant-matched vaccines should they be needed. We look forward to sharing data on our multivalent booster candidate, mRNA-1273.211, which combines mRNA-1273 and mRNA-1273.351 in a single vaccine, when available. We will continue to make as many updates to our COVID-19 vaccine as necessary to control the pandemic.
Moderna has three vaccines in its portfolio to release in the fall if they are approved. There will be new ones by next fall as new variants emerge and begin to circulate. The CDC will then be in a position where they have to manage SARS-CoV-2 the same way they manage the influenza viruses: surveillance monitoring, prediction, and formulation. This chart is CDC’s data on flu shot efficacy:
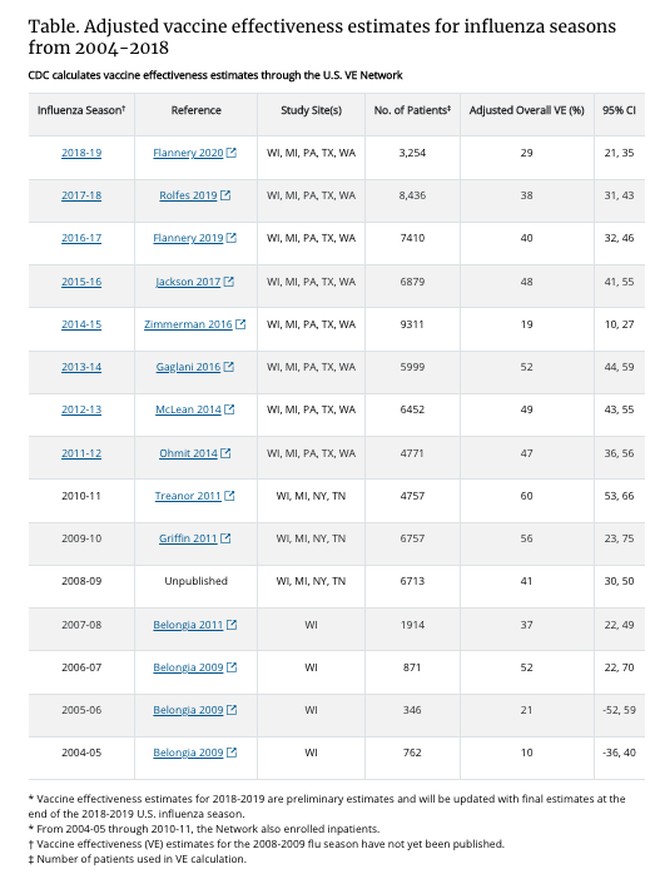
There is no planet where vaccine mandates or passports make sense for flu shots with that level of performance. It makes no sense in COVID-19 vaccines either. Like flu shots, they should be voluntary and focused on at-risk populations. Researchers from Emory University and Pennsylvania State University made this recommendation in February:
We are currently faced with the question of how the CoV-2 severity may change in the years ahead. Our analysis of immunological and epidemiological data on endemic human coronaviruses (HCoVs) shows that infection-blocking immunity wanes rapidly, but disease-reducing immunity is long-lived. Our model, incorporating these components of immunity, recapitulates both the current severity of CoV-2 and the benign nature of HCoVs, suggesting that once the endemic phase is reached and primary exposure is in childhood, CoV-2 may be no more virulent than the common cold.
Recommended: DeSantis Blasts Biden: ‘I Don’t Wanna Hear a Blip About COVID From You’
The paper went on to say:
Should the vaccine cause a major reduction in transmission, it might be important to consider strategies that target delivery to older individuals for whom infection can cause higher morbidity and mortality, while allowing natural immunity and transmission to be maintained in younger individuals.
Moderna’s press release and the data we see about the Delta variant certainly support this view. Like the flu and viral pneumonia, COVID-19 will find particular at-risk populations every year and cause severe illness and even death. However, mandates in a world of surveillance and prediction for vaccine development are absurd, especially if efficacy declines through the season. It is long past time our healthcare experts admit this and reset the expectations of Americans they have put into an unwarranted state of panic over the last 18 months.






