On March 21, 2020, President Donald Trump tweeted out a plea to the CDC and FDA to allow doctors to treat COVID-19 patients with hydroxychloroquine (HCQ) and azithromycin (AZT). Both are cheap and effective medications that the medical community had decades of experience using for various illnesses. Recently, another study demonstrated increased survival rates when HCQ was given in combination with AZT to those who were severely ill with COVID-19.
What should bother Americans is that this is not the first study that demonstrated the effectiveness of HCQ. According to a website that has been tracking studies on early treatments for COVID-19, there have been 255 studies globally that show significant improvement when HCQ is given early in the illness. The results should surprise no one.
In 2005, HCQ’s precursor with the same action, chloroquine, was found to inhibit the growth of SARS-CoV-1 in vitro. The researchers concluded:
Chloroquine is effective in preventing the spread of SARS CoV in cell culture. Favorable inhibition of virus spread was observed when the cells were either treated with chloroquine prior to or after SARS CoV infection.
Doctors now prescribe HCQ rather than the older chloroquine because it is a less toxic metabolite when taken long-term.
The study indicated that the drug could be used as a prophylactic or treatment for the original SARS. SARS-CoV-2, commonly called COVID-19, is 80% similar to SARS and uses the same receptor to enter human cells. It made sense that doctors, when confronted with the new strain, would look at the literature for SARS. French physician and microbiologist Didier Raoult was one of the first advocates for the use of HCQ in COVID-19. A researcher with 2,300 peer-reviewed studies under his belt, Raoult could not have predicted the damage this would do to his career.
On April 5, 2020, President Trump held the infamous press conference where he expressed optimism about HCQ and remdesivir. Dr. Anthony Fauci declared at the time that any evidence for HCQ was anecdotal, which was absurd. Competent physicians had observed its effectiveness in caring directly for patients by that point. The media’s wholesale campaign against the drug was insane. At the time, I wrote that the president has science on his side in having optimism about HCQ. In addition to the 2005 study on chloroquine, the mechanism of how the treatment, which included zinc, should work was pretty straightforward:
It [zinc] inhibits the replication of many types of viruses by interfering with RNA transcription. If you have ever taken Zicam for a cold over the counter, it is because we know it interferes with both the rhinoviruses and coronaviruses that cause the common cold. The NIH has also known since 2010 that it killed the SARS, another coronavirus virus, in a test tube. The COVID 19 coronavirus must also transcribe, or replicate, its RNA to survive. It’s this process the current protocol is meant to disrupt.
In layman’s terms, chloroquine or hydroxycholorquine holds the door to your cells open and carries zinc across the threshold. Once inside, if an RNA virus is present, zinc interferes with it making photocopies of itself and taking over the cell processes. This reduces the overall viral load inside the patient giving their own immune system time to mount a response to kill the virus.
The campaign against HCQ did not diminish, despite the simple pharmacology that applies to all RNA viruses. Instead, the media touted a horribly constructed study using lethal doses in severely ill patients as evidence against the drug. Then, an utterly made-up study was published in Lancet, which resulted in the cancelation of trials for the drug globally. Even when the fictitious research submitted by Surgisphere was retracted, the medication was dropped and denounced by the media.
Related: Trump Vindicated (Again) by New Study on Hydroxychloroquine
Dr. Harvey Risch, a respected Yale epidemiologist, almost had his career ruined for producing a meta-analysis of available studies on HCQ and asserting that he could not discount the benefits he found due to the statistical significance. Dr. Simone Gold lost her job for advocating for its use. Her entire organization, America’s Frontline Doctors, has been chased around the internet, with videos removed from YouTube and websites taken down by hosting companies. The state threatened Dr. Zev Zelenko’s license, while governors, medical boards, and pharmacy boards prohibited the drug’s use in COVID-19 patients.
These actions demonstrated unprecedented interference in a doctor’s right to prescribe off-label. And it was not limited to HCQ. Other medications—ivermectin and outpatient treatment protocols that use steroids and drugs to prevent blood clots—have also been censored. These are primarily inexpensive generic medications that doctors are using for recently hospitalized patients in early illness. Ivermectin, like HCQ, has dozens of positive studies, including 29 randomized controlled trials that show significant benefits.
Some of these doctors testified in front of the Committee on Homeland Security and Governmental Affairs when Senator Ron Johnson (R-Wisc.) was chairman. They begged for funds to do the studies the NIH required of them. Johnson inquired with the NIH, and the agency dismissed his inquiry. All the Big Tech platforms censored videos of the congressional testimony. Evolutionary biologist Bret Weinstein also had his podcast removed from YouTube when he interviewed Dr. Pierre Kory, an advocate of ivermectin,
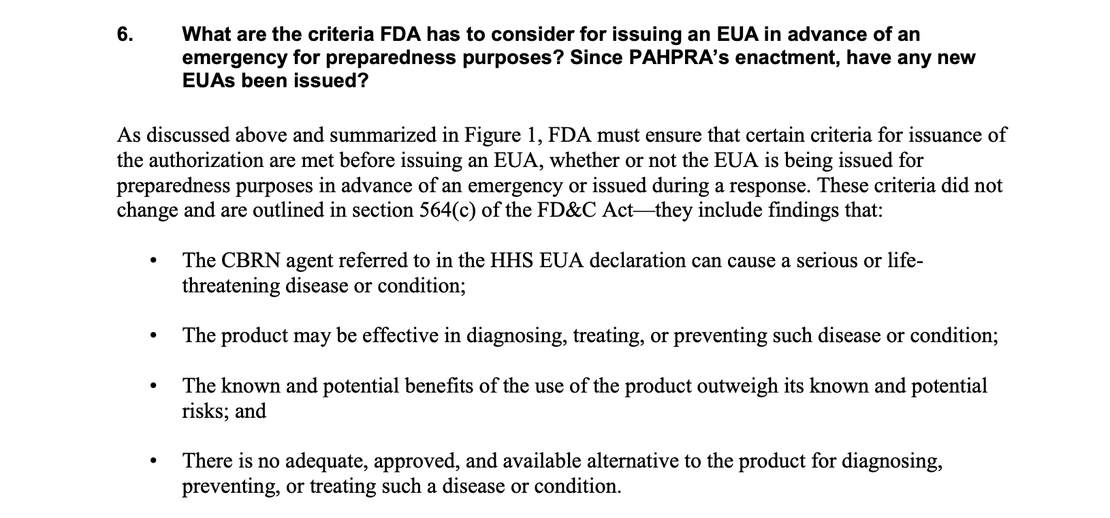
The obvious question is “why?” The answer is simple. Remdesivir, a failed HIV medication that costs over $3000 for a five-day course, might not have gotten an emergency use authorization (EUA) under the current rules if repurposed generics were deemed adequate. The FDA granted the remdesivir EUA after one flawed study that changed to outcome criteria:
Not to mention the fact that if people never went to the hospital, they never would have been prescribed the intravenous medication. Clinicians were focused on keeping people out of the hospital and doing it successfully with generic medicines.
Related: Why Are Inexpensive, Generic Outpatient COVID-19 Treatments Being Suppressed?
Clearly, the system for placing existing drugs on the list of NIH treatment protocols needs to change. As Weinstein asserted, “There is a safe prophylactic against COVID, and we aren’t using it because repurposed drugs are unprofitable and experimental treatments with EUAs are.” Given the price of remdesivir, this seems obvious. Perhaps a minimum number of random control trials of a repurposed generic showing benefit should mandate that the medication or combination be placed on the NIH treatment protocol. If remdesivir could earn an EUA with one garbage study, safe and effective repurposed drugs should not require very many.
Weinstein called the failure of the FDA and NIH to authorize these drugs for the treatment protocols “the “crime of the century.” Doctors advocating for early outpatient treatment estimate that these protocols could have prevented between 50-75% of deaths from COVID-19. Looking at the meta-analyses, this could well be the case. The part that should enrage everyone who lost a loved one or is suffering from long-haul symptoms is that no one will be held accountable. That is also something that must change.