
So there’s been another Ebola outbreak, this time in Congo. I’ve observed over the years that what radiation is to liberals, infectious diseases are to conservatives. I hope to head off some of the hysterics with this article, or at least have a link I can leave in comments so I don’t end up repeating myself. I’ll tell you frankly, a lot of this is cribbed from an article I wrote in the Great Ebola Panic of 2014-2015 that was never published.
Ebola is a scary disease, made much more scary by some wildly exaggerated claims in some books and movies. So, before we talk about Ebola, let’s talk about another scary disease called “rabies.”
It’s a virus, serum transmitted — meaning contact with blood, saliva, or other bodily fluids from an infected individual is needed to transmit the disease. Thousands of people die of it worldwide, every year. Once you’ve sickened with it, become symptomatic, the symptoms are pretty horrible, and there’s really no effective treatment. People who develop the symptoms are very likely to die.
In fact, the number of people who have survived active rabies can be counted on one hand with fingers left over.
Of course, people don’t panic over a case of rabies. Or maybe just a little if it turns out there’s been a rabies outbreak in a local prairie dog colony or raccoon population. During the last outbreak, I observed at one point that at least no one had suggested nuking Sierra Leone, as people were doing during the Fukushima accident. But it turned out I’d spoken too soon: people suggested exactly that.
There’s another similarity though: As with the Fukushima accident, the panic is a lot more dangerous than the disease itself.
Yes, Ebola is horrible
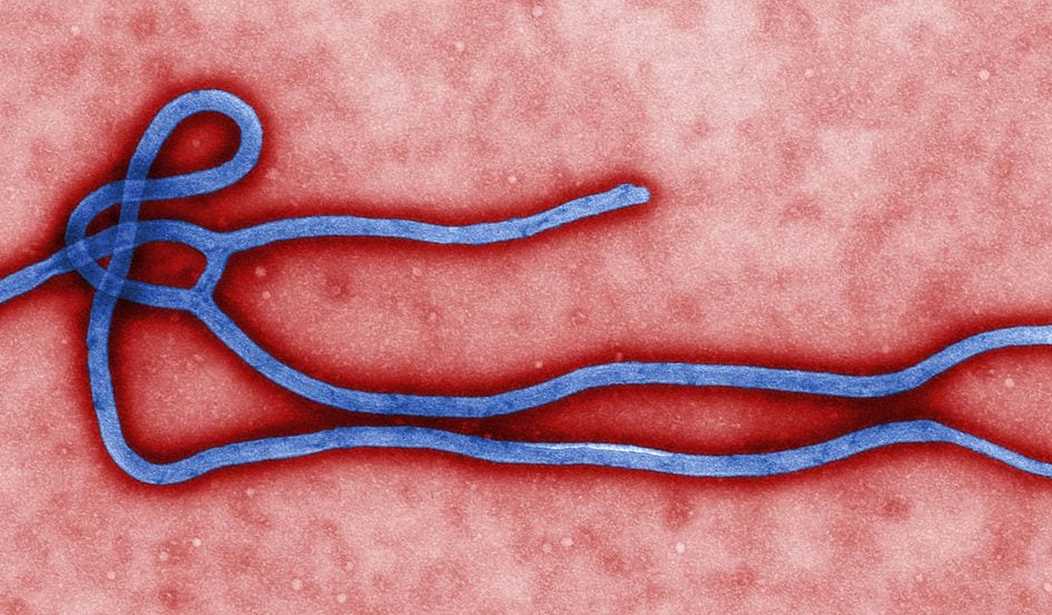
Ebola — strictly (Zaire) Ebola Virus Disease, and there are some technicalities in the name that aren’t very interesting — is a scary disease and horrible to have. It starts like the flu, with fever, weakness, body aches, and progresses to vomiting, diarrhea, chest and stomach pain, internal bleeding, and in some patients to bleeding from the eyes, nose, and anus, and then death.
Thoroughly unpleasant.
If you live in West Africa, where you are either treated by traditional medicine doctors or thrown out in the street, then the mortality — the proportion of people who will die — is as high as 90 percent. If you receive decent treatment in a modern hospital, the mortality is — well, apparently a lot lower. We don’t have a good idea how much lower, since the number of people who have been treated for Ebola in a modern hospital is really low. But it’s much lower.
But then, compare that with rabies, which causes dementia, convulsions, and yes, painful death. And the number of people who have survived rabies can be counted on one hand, with a finger or two left over.
Yes, Ebola is infectious — like rabies, HIV, and hepatitis
Like rabies, HIV, and hepatitis, Ebola is transmitted by serum — things like blood, saliva, and, well, other stuff. It’s not like, say, measles: it can’t be transmitted by simply spreading through the air. What can happen is that droplets can be spread or splattered, and if you come into contact with those droplets, you might be infected.
And again, compare this with rabies, which is also serum-transmitted. In general, if you avoid being bitten or scratched by a rabid animal, you can avoid getting rabies. Now, this doesn’t mean you can’t get rabies, in some sense, through the air. People who explore caves with big bat populations take great care to wear respirators to avoid exposure to rabies because bats do in caves what bears do in the woods. Kick up enough bat guano and you might be exposed to some rabies virus that’s still alive.
So people treating Ebola patients need to take fairly extreme measures to avoid coming into contact with live Ebola virus particles. They wear respirators and full-body protection, or even hazmat suits, and they’re very careful when they take the protection off so there’s no chance of contacting the outside of the protective gowns or suit. During the 2014/2015 outbreak, the first nurses who treated that first Ebola patient contracted Ebola themselves — they hadn’t gotten good advice on the protective garments and got exposed.
Of course, they both recovered. This is a fact we’ll come back to later.
No, Ebola isn’t terrifically infectious, especially compared to other diseases
There are diseases that are a lot more infectious than Ebola. Two of them are actually very common: measles and influenza. The degree to which a disease is infectious is expressed in a number called R0, “R nought,” the basic reproduction ratio. Without going into the differential equations, R0 equations can be thought of as the average number of new cases you expect from each untreated un-isolated case. This leads to a basic trichotomy:
- if R0 < 1, the infection will die out on its own
- if R0 = 1, the infection is “steady state”; as many people have it in the next generation as had it in the previous
- if R0 > 1, the infection will spread to more and more people until something else (like running out of people) stops it.
Some of you may remember a commercial — I found it, Faberge Organics Shampoo — where Heather Locklear tosses her hair while explaining the wonders of this shampoo, and then says: “So I told two friends, and they told two friends, and so on and so on and so on … ” while the screen fills with more and more, tinier and tinier pictures. (Mathematically, this is called a geometric progression.) In the commercial, Heather is “infecting” two friends with her shampoo preference; they infect two more friends, and — yes — so on.
This means Heather’s shampoo has an R0 of 2. This turns out to be an excellent example, because Ebola has an R0 of about 2.
But here’s the deal — something that’s really infectious, like Measles, can have an R0 of 18 in an unvaccinated population (like my 4th grade class). If Heather’s shampoo were as infectious as measles, then she’d be telling 18 of her friends.
(I can’t resist a little aside here. This is why “herd immunity” works: under the covers, R0 is a measure of how probable a new infection is when an infected patient encounters someone who isn’t immune. When you have a successful vaccination program, the probability of encountering someone who isn’t immune is very small, so R0 is much less than 1. The infection doesn’t spread.)
So Ebola is nine times less infectious than Measles, but that doesn’t tell the whole story because the actual number of infections is growing exponentially. With Ebola, the number of infected patients after k generations is 2k; with measles it’s 18k.
This is a big difference: after 19 generations, Ebola can only infect about 525,000 people. After 19 generations, how many could measles (theoretically) infect?
708,235,345,355,338,000,000,000
That’s 708 septillion. Of course, that’s silly — you run out of people who could possibly be infected around the eighth generation.
What makes Measles so much more infectious than Ebola? Measles is spread through the air easily. Cough or sneeze and little Measles virus particles float through the air for hours, even days.
No, Ebola is not likely to become airborne
This is one of those times when science-talk really interacts badly with journalist-talk. Ask an expert about the possibility of Ebola mutating to become airborne, and almost no one will say “no it’s absolutely not possible.” In science, the probability of something like that is never exactly zero.
In the case of Ebola, it is, however, very unlikely. To see why let’s talk about how viruses work. If you are a virus, a cell is about the size of a football stadium, and like a stadium, the cell has a whole bunch of entrances — called binding sites — scattered around it. This is how a virus works: it has a protein that can bind to one of these binding sites that are normally used for something else. It’s like it somehow gets a master key that lets it open the doors from the loading dock.
If the virus bumbles past and finds a door it can open, it does, and that’s when the fun begins: the virus gets into the cell and starts replicating, using the resources of the cell to do so. This is great for the virus, not so much for the cell.
The thing is, the virus doesn’t have a master key for every kind of lock there is. It can only bind to certain proteins, and those proteins are different for different kinds of cells. It’s like if people who build soccer stadiums usually buy their locks from different companies than the people who build football stadiums.
Ebola, it turns out, can bind to a lot of kinds of cells. But it has strong preferences for cells inside the body, specifically cells that line the blood vessels. Lung cells and such have different locks. And the skin is covered with dead cells that are no use at all.
The point here is that a virus isn’t like a bulldozer, plowing its way in; it needs a door it knows how to open.
Mutation can change the keys, but it takes a lot of mutations to make a whole new set of keys — it’s a lot easier to get from one Kwikset key to another than it is to turn a Kwikset key into a key for a Master padlock.
In fact, in the roughly 100 years that viruses have been studied, no virus has ever changed its mode of transmission.
Do you lie awake worrying that rabies is going to become airborne? That would be scary: if it were, you wouldn’t know you had it until you showed symptoms, and at that point it’s pretty certainly too late.
Beyond the fact that the mutation thing is very improbable, Ebola viruses are unusual: they’re big. An Ebola virus may be 80 nm in diameter but they can be as much as 14,000 nm long — or, if you’d rather, 14 µm. By comparison, an influenza virus is only about 10 nm. HIV, which also doesn’t transmit through the air very well, is about 10 times that, 100 nm. In other words, if flu is the size of a marble, HIV is the size of a tennis ball. Ebola is as long as a bus.
So what should we do about Ebola?
There’s a reason I’ve used rabies as a comparison: it’s got a similar method of transmission, it’s got a similar incubation period, and frankly the likely outcomes for someone who is actually infected are much worse. And what we should do about Ebola is roughly what we’d do if someone shows up with an active case of rabies.
We try to immunize everyone who might be exposed. This is a big difference from the 2014/2015 outbreak: we actually have an effective, albeit still officially experimental, vaccine. (That last link is to the Lancet paper, and it has something I’ve never seen on a scientific paper before: the title ends with “Ebola Ça Suffit!”)
We’d isolate them in a hospital. Yes, we’d want to keep them in isolation, but this kind of isolation is done all the time. (And yes, if you’ve been following this at all over the years, you will have seen people saying they shouldn’t be treated, just as there were people saying the doctors who got it in Africa shouldn’t be allowed to get the best treatment here.) Treating the patients is a lot easier now that there’s an effective vaccine: you don’t need to worry nearly as much about accidentally breaking protocol if you’re unlikely to catch the disease.
We would track down everyone who could have been exposed. This is called contact tracing and it’s something that public health people do all the time. (Show up at the doctor with measles, chicken pox, or whooping cough, and the Health Department will ask you a lot of questions.) We would then try to vaccinate them and pretty much everyone around them.
Contact tracing is actually somewhat easier with Ebola because Ebola has such a quick onset — once you start getting sick, you get really sick really fast, and you’re not contagious until you’re actually sick. With rabies, there’s an interval in which you can be contagious but not be noticeably sick yet.
Having found those people, we would keep an eye on them. Some people who are most likely to have been exposed might be quarantined, but even that is just being extra cautious. Remember, with Ebola, if you’re not sick, you’re not contagious. Now, anyone who develops a fever or flu symptoms among those contacts can pretty well bet they’ll be in isolation too, but as long as you do that until you determine if the person really has Ebola, you can pretty well nip the whole thing in the bud.
Follow Patton’s Advice and “take not counsel of your fears.” Ebola is scary, but panic is, in itself, a risk: the worse it gets, the more people who fear they might get Ebola will try to go underground, the more everyone else’s life will be disrupted, and the more likely an Ebola patient will come into contact with unvaccinated people.
Global Warming, Fukushima, and Ebola
One of the first big science stories I covered at PJ Media, back in the pajamas days, was the release of the Climategate files. I’d been following the climate change science for quite a while; the hysteria behind that was, of course, pretty pronounced at the time. It had become clear even then that there were a lot of people in the UN and third-world countries — and not a few in the U.S. — who saw it as a combination gravy train and political cudgel. This has been helped along for a very long time by poorly informed journalists falling for the most catastrophic worst-case predictions, often ones that basically didn’t even make sense.
The solution, as always, is to give the government more power while accusing anyone who disagrees of having been paid off or otherwise having an ax to grind.
Of course, the science isn’t standing up, and now the riders on that gravy train are being forced into trying to silence critics and threaten skeptics to keep it going. Science is like that: try as you might, the process eventually shows the holes in any hypothesis.
In 2011, a combination of a force-9 earthquake and a thousand-year tsunami caused a reactor accident and meltdown at the Fukushima Daiichi plant. As we have reported ever since, this also led to lots of hysteria — remember when the fallout was going to kill everyone on the West Coast? It comes back every so often; last year it was the “radioactive plume in the Pacific Ocean.”
The panic then was, once again, largely coming from poorly informed journalists who frankly weren’t real clear on long division, again listening to the most absurd worst-case predictions from people who often had hidden motives. (My first piece on Fukushima was called “Fear the Media Meltdown, Not the Nuclear One.”) And the solution was, as before, the suggestion that the government should have more control, should forbid nuclear power, and anyone who disagreed was accused of being in the pay of the nuclear power industry or having an axe to grind.
Once again, the science didn’t stand up. The massive radiation release turned out to be bad enough, but the killing fallout of 2011, and the massive radiation plume of last December, didn’t happen.
Now, we’ve got Ebola again. Just like the last time, people are panicking. (Just look at the comments on the Instapundit post about the new Congo outbreak.)
Sure enough, the solution once again is to give the government more power — close airports, stop flights, restrict Americans from going there and Africans from coming here.
This time, like the others, the science doesn’t stand up. But a crisis is a horrible thing to waste.





Join the conversation as a VIP Member